High cholesterol has long been linked to heart disease, but much of what people believe about cholesterol is based on myths and outdated information. This confusion can lead to poor dietary choices, unnecessary anxiety, or neglect of critical risk factors. This article sheds light on ten common myths about cholesterol and heart disease, separating fiction from reality to help you make informed, heart-smart choices. Each myth is countered with clear, science-backed facts to empower you with accurate knowledge.
1. Myth: “All cholesterol is bad for your heart.”
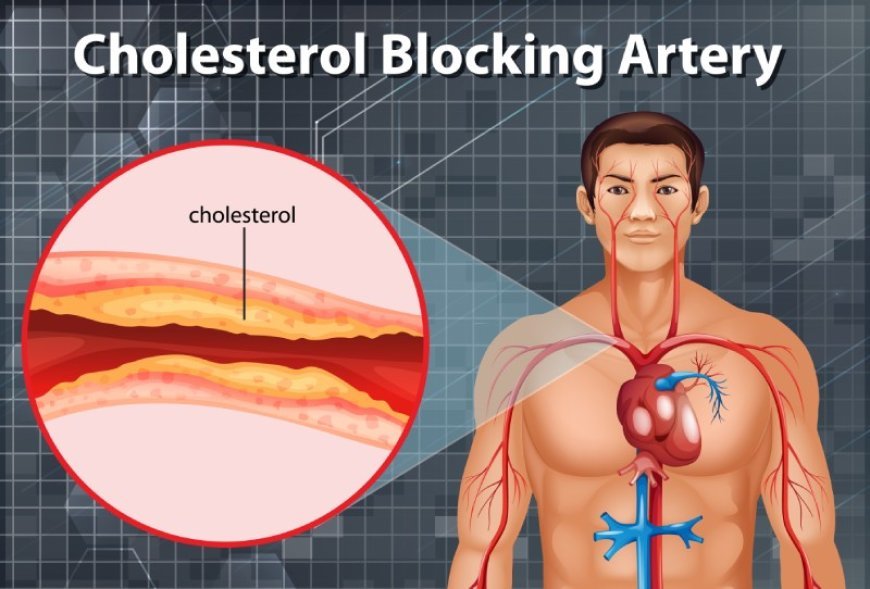
Many people assume that any source of cholesterol automatically puts them at risk for heart disease. The truth is more nuanced. Our bodies need cholesterol: HDL ("good") cholesterol helps clear LDL, while LDL ("bad") cholesterol can lead to arterial plaque buildup. The problem arises when LDL levels become too high, especially when oxidized, and HDL is low. Focusing on overall cholesterol levels without considering their subtypes can obscure important nuances.
Continue reading this piece by leonard
Join our community to access the full story. Creating an account is completely free and only takes a moment.
- Read unlimited free publications across the platform
- Directly support independent journalists and authors
- Join discussions, leave reactions, and save your favorites











Responses (0)
Sign in to share your thoughts.
Sign in